Vestibular assessment
The videonystagmography has revolutionized neurotology: goggles with an infrared camera are placed over the patient’s eyes, to view on a screen and measure eye movements that are either spontaneous or induced in the dark by various tests.
Testing for nystagmus in the dark
The aim of the clinical examination is to detect the presence of nystagmus, which would indicate vestibular asymmetry. Nystagmus involves slow eye movements with rapid intermittent phases in the opposite direction.
For diagnosis, the patient must be sitting and then lying down with videonystagmoscopy goggles, thus being placed in the dark to prevent inhibition by fixation. The goggles are equipped with a camera and monochrome infrared light, and the idea is to detect the iris imprint. A 3D study of the components of spontaneous nystagmus is essential. Is the nystagmus horizontal or vertical? Is there a torsional component? Is it inhibited by ocular fixation? Lastly, is it triggered by certain head movements?

Testing for positional nystagmus
Patients are placed on their side, the head tilted upwards and rotated 45° to the left and right. This movement helps to detect positional vertigo resulting from the displacement of otoconia or small crystals in the inner ear.
In practice, the patient experiences significant rotational vertigo when lying on either side. The nature of the eye movements and especially their vertical or torsional direction will indicate which ear is affected and guide the practitioner’s liberatory manoeuvre, which is necessary to rid the patient once and for all of this disabling vertigo.

Head shaking test
The patient's head is turned horizontally for 20 seconds with their eyes closed. Afterwards, in normal patients, nystagmus is not triggered. With patients suffering from a condition affecting the inner ear, nystagmus is observed and indicates a lesion of the inner ear on one side. See the video below:
Vibration test
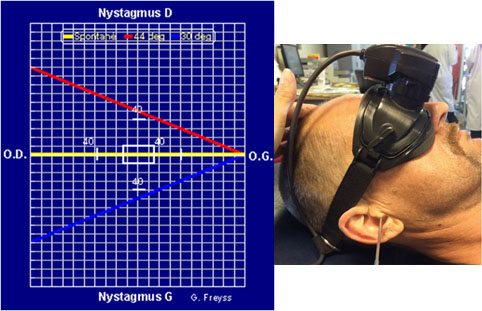
The vibration test is to detect an asymmetry in the vestibular system at high frequencies. A 100 Hz vibrator is applied in sequences on the left and right sides behind the ear (behind the mastoid process) for 3 seconds.
In patients suffering from vestibular asymmetry, this test induces nystagmus, that is to say slow eye movement with intermittent rapid movements towards the affected side.
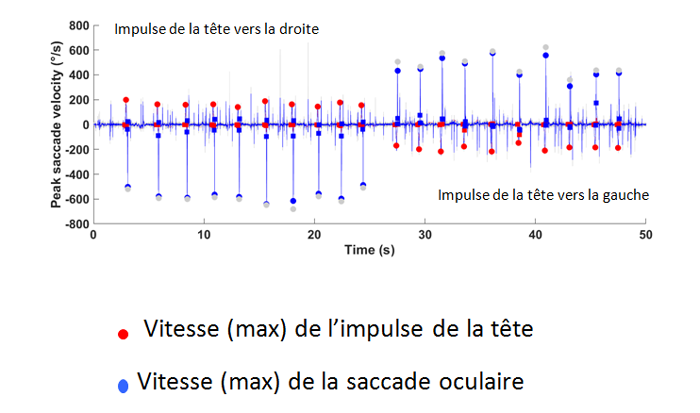
Head Impulse test (HIMP)
The Head Impulse Test is a new horizontal vestibular canal function test. It is used to detect a peripheral vestibular deficit in the horizontal and vertical planes.
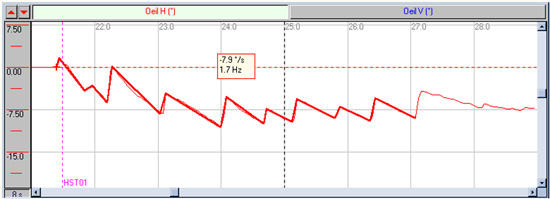
In practice, the patient’s head is turned rapidly, on average at a speed of 200°/sec, either to the left or right, while the patient is instructed to fix their gaze on a target 91 cm in front of them (see figure). The patient wears goggles to measure 1. the head speed and 2. the speed of eye movement.
If vestibular function is normal, the eyes move in the opposite direction to the head but at the same speed. The horizontal vestibular ocular reflex gain is close to 1.
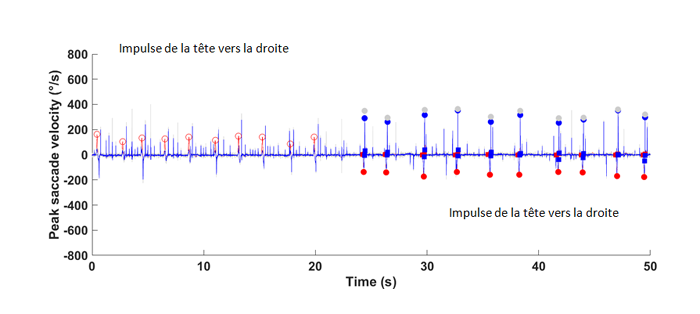
If vestibular function is abnormal, patients produce catch-up saccades as they deviate from the target: the eye movement is slower than the head movement. The gain is less than 0.8. Catch-up saccades can be early (covert saccades) or late (overt saccades).
This test can be performed in the horizontal canal plane or the vertical canal planes. It is easy to perform, non-invasive and painless. The test is sufficient if it shows a dysfunction and avoids the need for caloric tests.
These innovative tests developed by Professors Curthoys and Halmagyi (Sydney, Australia) are a way of quantitatively testing both the horizontal and (anterior and posterior) vertical canals of the inner ear.
Disorder Normal
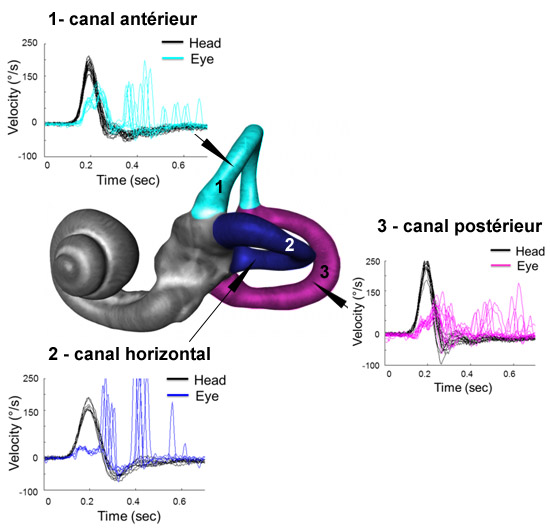
v-Head impulse testing of the three semi-circular canals in a patient after surgery for a left vestibular schwannoma
Caloric tests
Described for the first time by Bárány, these tests serve to assess and compare the sensitivity of both inner ears (ampullae of the horizontal semicircular canals).
In practice, hot water (44°C) or cold water (30°C) is applied to the left or right external auditory canal for 20 seconds. This irrigation activates (hot water) or inhibits (cold water) the inner ear and causes a rotational sensation lasting one to two minutes. The eye movements induced are measured in the dark using a videonystagmography. The responses on the left and right are then compared, to detect a problem with the inner ear.
In addition, these tests allow patients to specify the sensation experienced, which reflects the central integration of vestibular information. The absence of any sensation can be observed among elderly patients, which indicates a dysfunction in the cortical areas involved in processing information from the inner ear.
SHIMPs ou Suppressive head impulse paradyme
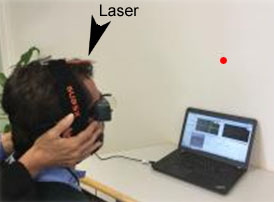
The patient’s gaze must follow the moving laser pointer while the examiner rapidly moves their head to the right or left (acceleration 4,000 to 8,000°/sec). If the vestibular system function is normal, the vestibular ocular stabilization reflex causes the eyes to move in the opposite direction to the head movement (horizontal vestibular ocular reflex). The patients have to produce a catch-up saccade to keep their gaze on the laser. Conversely, if the vestibular system is not working, the eyes remain still and look at the laser target. The examiner will not see any saccade.
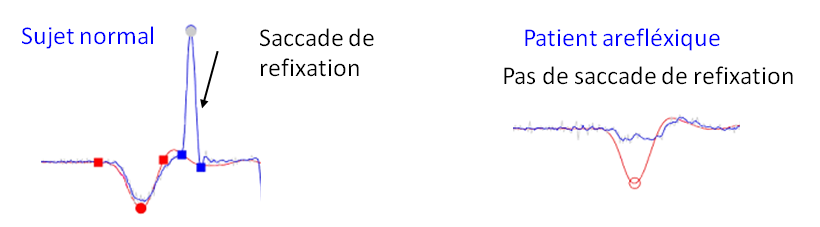
In normal patients, the head impulse generates a catch-up saccade to look at the laser target regardless of which way the head is turned.
In patients with a left reflex deficiency, the head impulse does not generate a catch-up saccade.
In conclusion, this test provides important information about residual vestibular function and the potential use of the saccade system to compensate for the defective vestibular system. It may be useful in patients suffering from oscillopscia (i.e. oscillations in the visual field caused by head movement).
Rotational tests
The patient is placed on a chair that rotates at a constant speed after an initial acceleration, and the eye movements are measured during and after rotation. This tests the functioning of both inner ears.
The chair rotates horizontally for one minute. For 4 seconds it accelerates from 0 to 80°/sec then rotates at a constant speed for 60 seconds before decelerating over 4 seconds from 80°/sec to 0°/sec. This test measures the time constant of the vestibulo-ocular reflex and detects in particular any asymmetry between the semicircular canals of the inner ears.
This examination is very well tolerated and non-invasive.
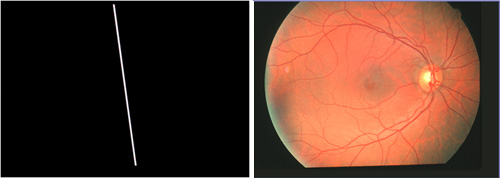
Subjective vertical perception test
This test serves to assess how well the otolithic system functions. It consists in asking the patient, in the dark, to place a 60 to 90 cm luminescent bar that is 1 m in front of them and at a 45° tilt, in a position that they believe is vertical. When there is an acute unilateral problem with the otolithic receptors of the inner ear, the patient places the bar in a position that is off-horizontal or off-vertical by around 3 to 15° on the damaged side.
Otolithic evoked potentials tests
These new tests to explore the inner ear are essential for diagnosing the cause of the problem. They test the functionality of receptors so far unexplored, which may explain the symptoms mentioned by the patient.
1. Cervical evoked myogenic potentials induced by high level sound (cVEMP 100 Db Hl) stimuli in the cervical muscles stimuli (or sacculo-spinal-induced otolithic evoked potentials)
Clicking sounds or short tone bursts of 100 dB are delivered on one side using a helmet at a frequency of 5 Hz, and cervical myogenic evoked potentials are received on the same side in both sternocleidomastoid (SCM) muscles using surface electrodes placed on the upper third of these two muscles.
The early waves are comprised of a first positive wave after 10 ms (P13 wave) followed by a negative wave after 19 ms (N23 wave).
These waves demonstrate the correct functioning of a labyrinth receptor, the saccule and saccular nerve, a branch of the vestibular nerve (inferior branch).

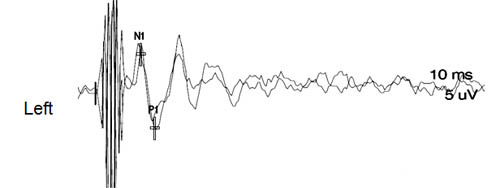
2. Ocular evoked myogenic potentials induced by high level sound stimuli (oVEMP or utriculo-ocular-induced otolithic evoked potentials)
Strong sounds are delivered in each ear and the evoked potentials are collected using surface electrodes on the extraocular motor muscles on the opposite side (n1-p1 waves). Bone conductive stimulation using a 4810 vibrator at Fz or at the mastoid evoked also n1-p1 potentials and may be useful in case of bo bilateral response due to decreased sensitivity of this test with age.
This new test serves to assess the functioning of the utricle and utricular nerve, comprising the superior vestibular nerve.

Testing for balance disorders
Balance disorders (feeling of inebriation, unsteadiness, tipping) are common with vestibular problems. They can be quantified with the help of fixed or moving platforms using static and dynamic posturography methods.
Fukuda test
The patient is asked to march on the spot (50 times) with their index fingers pointing forward. A normal patient will show no postural deviation.
If there is vestibular asymmetry, the patient rotates at varying angles greater than 30°, to the right or the left.
EquiTest®
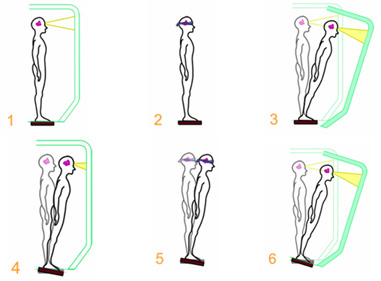
This apparatus is used to test the patient’s static and dynamic balance. It includes two main types of tests: a sensory organisation test and a motor control test.
The sensory organisation test explores the effect of six different sensory environments on postural control. To this end, the EquiTest includes a forceplate that is fixed or that follows the movements in the patient’s centre of gravity, and a visual surround placed 50 cm from the patient, which may be fixed or follow the movements in the patient’s centre of gravity.
The motor control test observes the latencies of postural responses to forwards-backwards or angular platform movements. It compares postural responses, taking into account the patient's age.
The EquiTest is a valuable tool to help appreciate and quantify balance problems and facilitate diagnosis. It also helps to guide vestibular rehabilitation and assess its effectiveness.
The moving platform
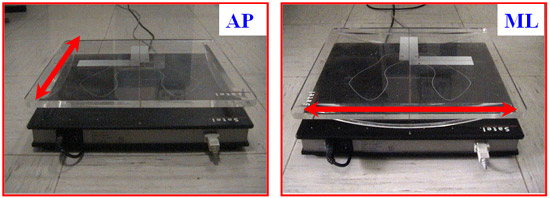
Patients are placed on a platform that tilts backwards and forwards and side to side.
Patients with unilateral vestibular lesions are more unsteady when rocked from side to side than backwards and forwards (Mbongo et al 2005).